We are measuring thetruenessbetween intraoral scanning (IOS) and conventional impressions of edentulous arches.
The problem is that, in this context (edentulous arches), trueness does not exist.
This is not a provocation: it is a methodological issue.
And from this misunderstanding arises a good part of the confusion — and the questionable conclusions — present in the literature.
The starting point: what is trueness really?
Truenessis defined as:the closeness between a measurement and the “true value”
This implies an essential condition:
👉 there must be a real, stable, and independent reference
In the case of edentulous patients, this assumption is simply not met.
The biological knot: soft tissues do not have a “true” shape
For edentulous arches, both intraoral scanning and conventional impressions replicate deformable soft tissues
And these tissues:
do not have a unique geometry they depend on the technique used
There is no single biological “ground truth”
change their shape under the pressure applied by the
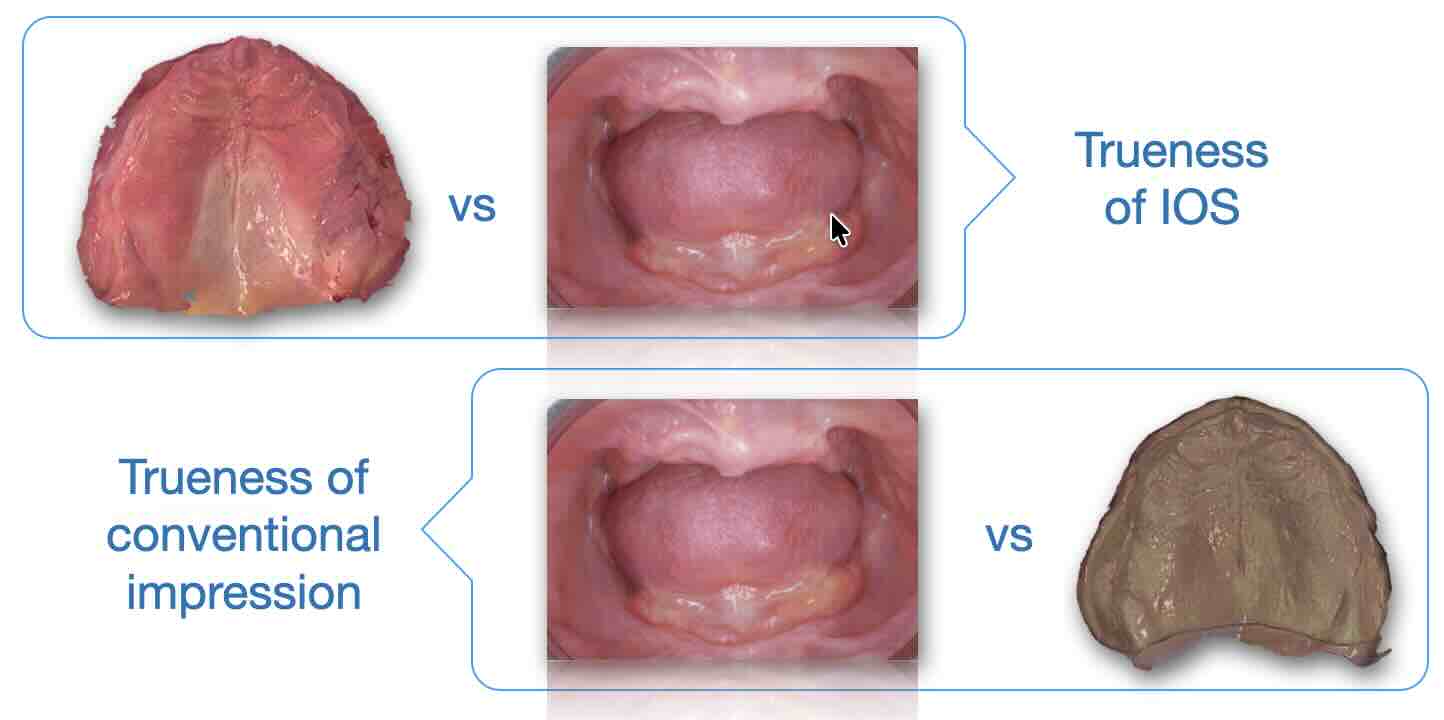
What are we really measuring in studies?
When a study compares IOS and conventional impressions, what it obtains is:
👉 There is no single biological “ground truth”
What are we really measuring in studies?
When a study compares IOS and conventional footprint, what it gets is:
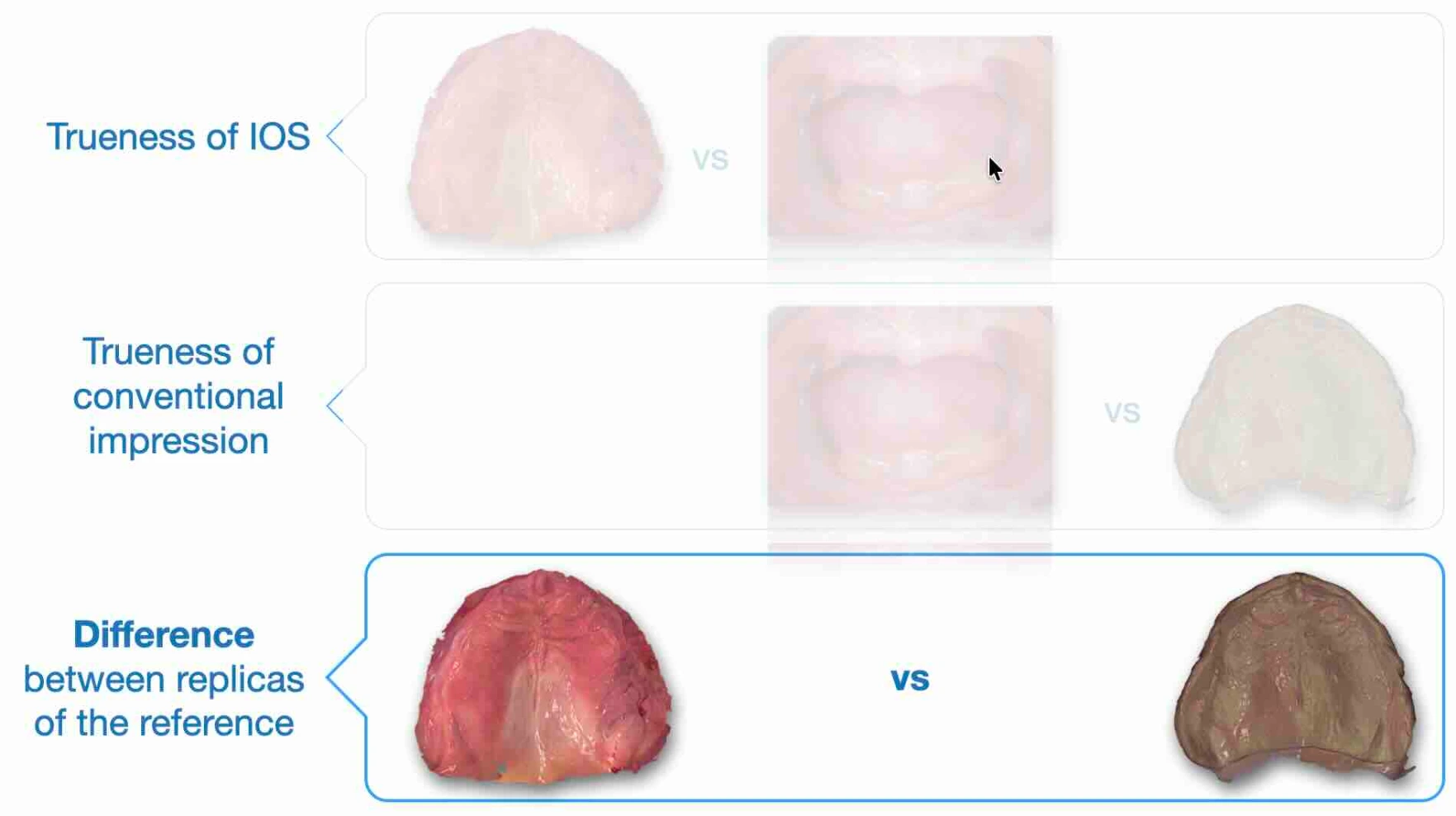
👉 the difference between two representations
Not the trueness. It seems like a semantic nuance. It is not.
The most widespread misunderstanding
That difference is often interpreted as:
👉 “error of intraoral scanning”
Here lies the logical leap:The difference we observe is not an error.
It is the inevitable result of two different ways of interacting with the tissue.
Two approaches, two realities: mucostatic vs mucocompressive
The point is not technological. It is biological.
Intraoral scanning
acquisition in the absence of pressure
tissues at rest
👉 mucostatic approach
conventional impression
compression of tissues
functional modeling
👉 mucocompressive approach
The consequence we often ignore
Expecting these two techniques to produce the same geometry means assuming that:
👉 soft tissue behaves like a rigid solid
It does not.
It is like comparing two photographs of the same object:
one without load
one under deformation
E poi chiedersi perché non coincidono.
Clinical implications: we are asking the wrong question
The dominant question in the literature is:
❌ “how much do IOS and conventional impression differ?”
But it is a less useful question.
The correct question is:
✅ “what tissue behavior do I want to record?”
mucostatic?
mucocompressive?
Because this changes the interpretation of the data
If we change perspective:
the difference stops being a problem
it becomes aconsistent consequence of the clinical choice
👉 Non è un limite della tecnologia
👉 it is a property of the method
The myth of the unreliability of intraoral scanning
Part of the literature concludes that IOS is:
“less reliable for removable prosthetics”
But often this conclusion arises from:
comparison with compressive impressions
misuse of the concept of trueness
interpretation of the difference as an error
transfer of principles from the mucocompressive philosophy to the mucostatic one
👉 It is not the technology that is unreliable.
It is the way we are asking the question.
A necessary paradigm shift
Continuing to numerically compare IOS and conventional impressions leads to:
data that are difficult to interpret
contradictory conclusions
unaware clinical decisions
The key point is another:
👉 stop looking for equality between methods that arise differently
And start consciously choosing:
what tissue behavior I need
Conclusion
The literature has tried to apply the concept of trueness to a context in which:
👉 there is no single geometric truth
This has generated:
misleading interpretations
criticisms that are not always justified
clinical confusion
The reality is simpler — and more useful:
👉 we are not comparing accuracy, but two different biological models
And as long as we continue to ask the wrong question,
we will continue to get irrelevant answers.
👉 Do you really want to understand when to choose mucostatic or mucocompressive - and how this affects the prosthetic outcome?
Dive deeper in our video course: Mucostatic vs Mucocompressive...
If you want to go deeper
If you want to see how these concepts translate into clinical practice:
/en/blog/intraoral-scanning-1/intraoral-scanning-edentulous-arches-2
Common errors in intraoral scanning of edentulous patients: guide to avoid them