Introduction
Intraoral scanning of edentulous arches does not present the same difficulties in the mandible and maxilla.
Although both represent toothless surfaces, the different anatomical and functional characteristics of the two arches, and especially the surrounding tissues, significantly influence:
scanner accessibility
tissue stability
scan extent
final accuracy of the acquired data
Understanding these differences is essential for adopting correct clinical strategies and achieving predictable results.
Why do the edentulous maxilla and mandible behave differently during intraoral scanning?
The two arches have profoundly different anatomies.
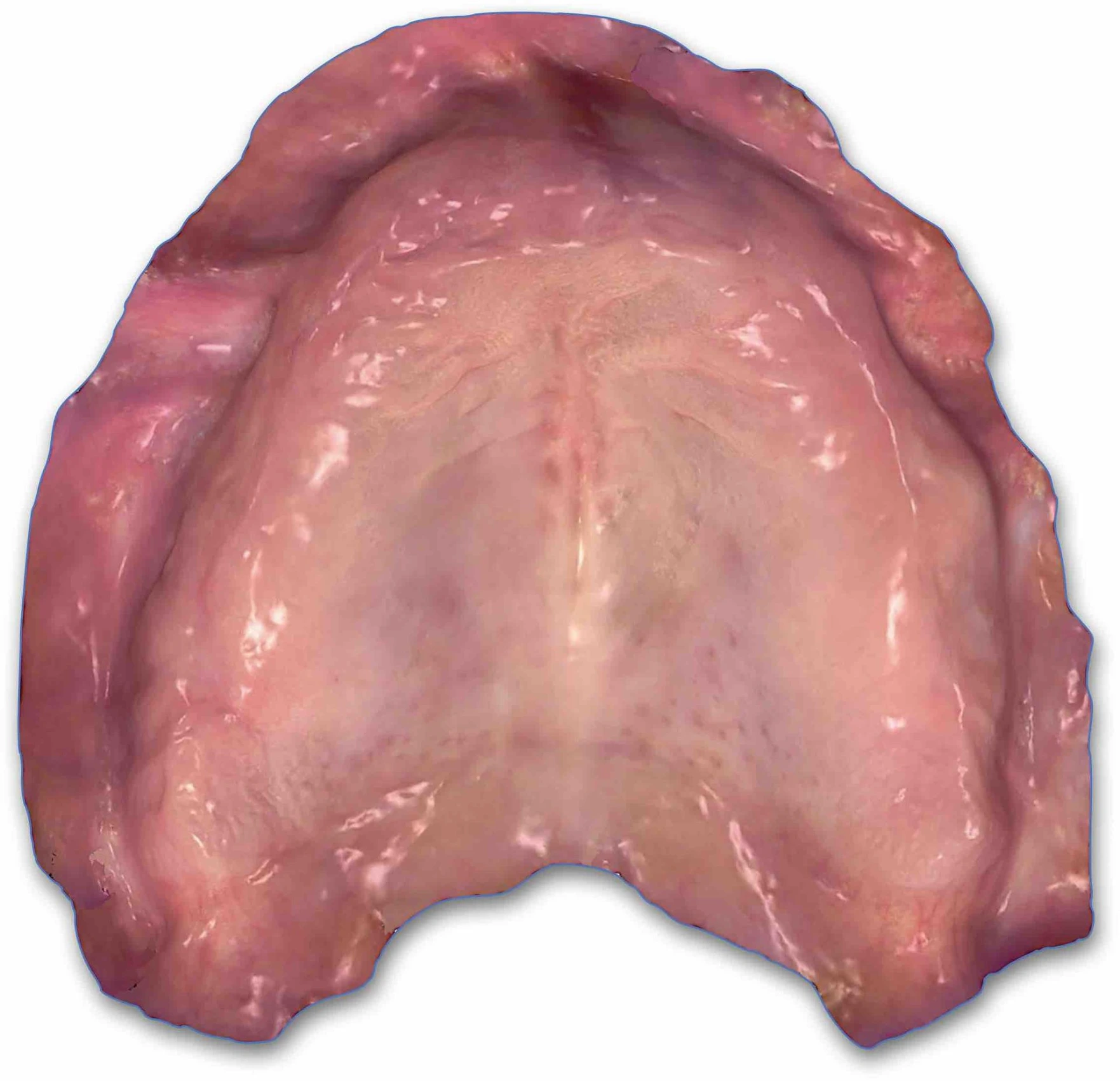
Maxillary Arch
The maxilla generally offers:
a wider and continuous surface
the presence of the palate as an area of anatomical support
less interference from the tongue
relatively more stable vestibular tissues
These characteristics tend to favor scanning, also considering the anatomy of the palate and the presence of palatine rugae.
Mandibular Arch
The mandible, on the other hand, presents greater challenges:
a more limited operating field due to more or less extensive resorption of the residual ridge
constant interference from the tongue
high mobility of the floor of the mouth
presence of the retromolar region
vestibule often reduced in depth and difficult to reach and control
👉 For these reasons, mandibular scanning is generally considered more complex.

The main challenges in scanning the edentulous mandible
Instability of soft tissues
Mandibular tissues are often:
mobile
compressible
easily dislocatable by muscle movements
This makes it more difficult to acquire a stable and repeatable surface and avoid incongruences and blocking in image stitching, especially in the presence of concurrent procedural errors.
Interference from the tongue
The tongue represents one of the main clinical obstacles:
it reduces accessibility
continuously alters the scanning field
compromises visibility of the posterior regions
Access to the retromolar region
A complete recording of the edentulous mandible often requires the acquisition of the retromolar region, a fundamental area for many removable prosthetic rehabilitations.
This region is:
deep
dynamic
difficult to access without adequate retraction
Specific challenges of maxillary scanning
Although generally simpler, maxillary scanning also presents some issues.
Extension of the palate
The wide and relatively uniform surfaces of the posterior palate can:
reduce geometric references
increase the risk of stitching error
Posterior vestibule and tuberosity
The correct acquisition of the posterior areas requires:
adequate tissue retraction
correct scanner inclination
humidity control
Accuracy: are there differences between the maxilla and mandible?
Clinical studies show that both arches can be scanned with high accuracy when:
validated scanning strategies are usedthe
The observed differences do not depend so much on the arch itself, but on the difficulty of managing the operating conditions.
Clinical Strategies for the Mandible
To improve mandibular scanning, it is advisable to:
Stabilize the pericrestal tissues
Reduce tissue mobility during acquisition.
Effectively retract the tongue
Completely clear the operating field.
Learn how to effectively stabilize and retract tissues with the Lo Russo Retractors® system
Use validated scanning strategies
Discover all the details of the scanning strategies for edentulous arches in our free video course!
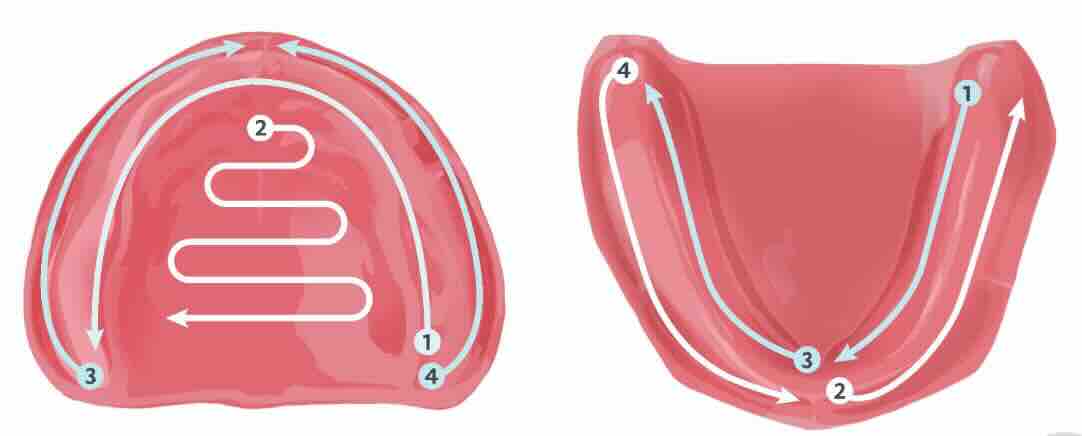
For example, scanning the edentulous mandible requires a two-step scanning strategy to allow for proper control of the tongue.
Clinical Strategies for the Maxilla
For maxillary scanning, it is useful to:
Correctly segment the scanning path
Avoid overly long paths on uniform surfaces.
Carefully manage the palate
Maintain continuous references and overlap between acquired and to-be-acquired tissue during the scanner's movement.
Ensure complete vestibular retraction
to properly capture the fornices and tuberosities.
Conclusions
Intraoral scanning of edentulous arches requires different approaches for the maxilla and mandible.
In summary:
the mandible presents greater operational difficulties
the maxilla generally offers more favorable conditions
both can be scanned accurately if clinical conditions are properly controlled
👉 The success of the procedure depends not on the arch itself, but on the ability to create optimal scanning conditions.
Improve control of intraoral scanning conditions with the Lo Russo Retractors® system