Intraoral scanning of edentulous arches, or very large edentulous saddles, is a very relevant procedure from a clinical point of view in both removable and fixed prosthetic rehabilitation. In fact, the direct digitization of anatomical data provided by intraoral scanning allows for the creation of an entirely digital environment where neither impressions nor physical models are required, making it possible to improve in terms of efficiency, effectiveness, quality, comfort of clinical procedures and laboratory.
Currently, there are still some doubts about the acquisition of edentulous arches using an intraoral scanner, both in terms of feasibility and accuracy. The reason most frequently reported as the cause of these concerns is the absence of "features". In reality, the three-dimensional development of the edentulous ridges offers macroscopic geometric characteristics (e.g. concavity, convexity) and widely scannable surface textures, as can be seen in the following image where the scan of the tissues of the hard palate and soft palate is represented.
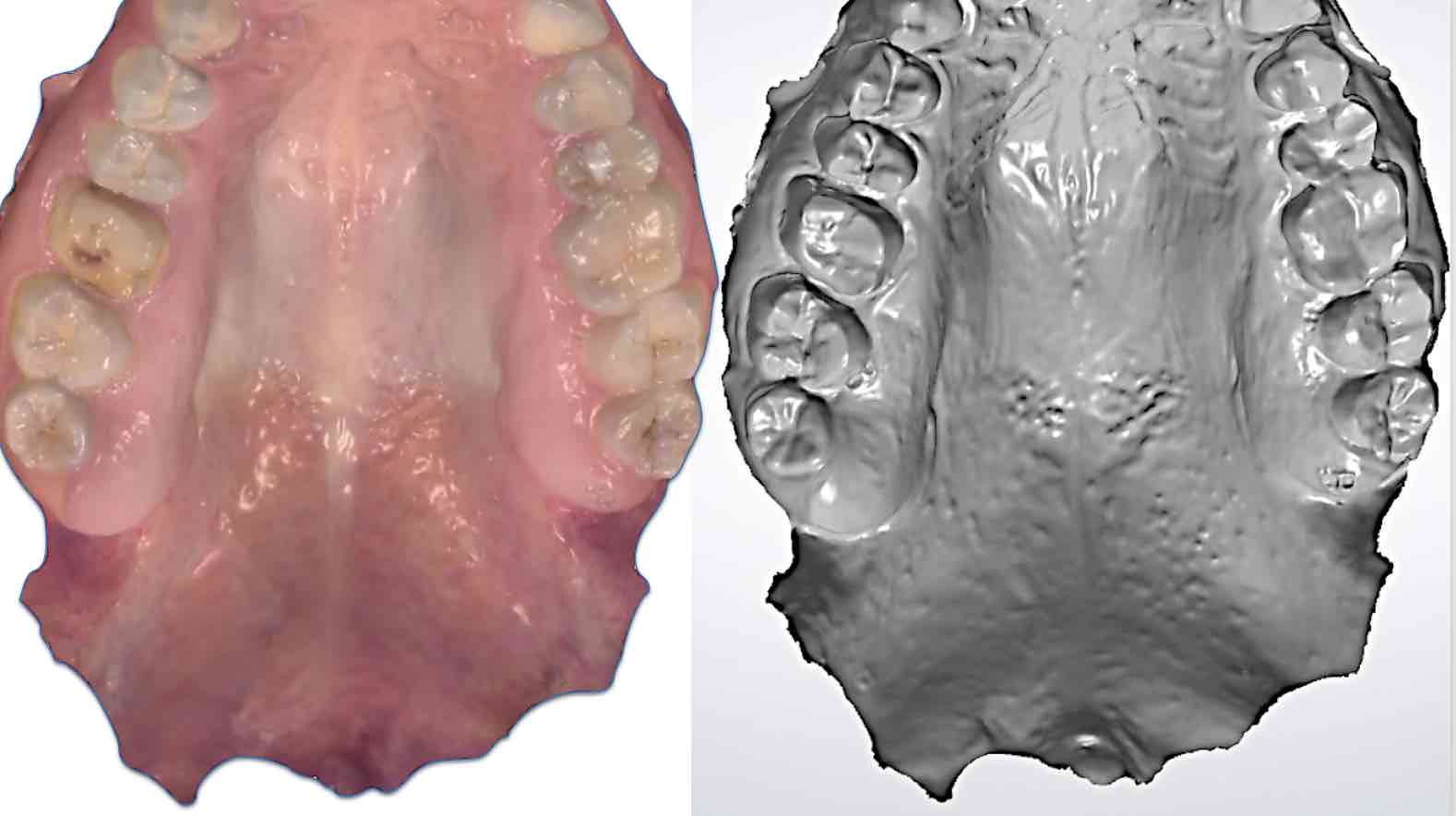
Figure 1: Scan of the soft palate; color manipulation makes macroscopic features and surface texture more evident.
Despite these findings, in order to improve the feasibility and predictability of intraoral scanning of edentulous arches, it has been suggested to add landmarks (cements, composites, or more complex structures); however, the usefulness of such an approach has never been demonstrated and remains, in all likelihood, an inappropriate complication of the scanning procedure.
It is clear, on the other hand, that intraoral scanning of edentulous arches can offer different levels of complexity and require a certain learning curve; however, it represents an opportunity for multiple clinical indications, widely feasible and achievable with suitable technologies and in adequate conditions. Let's try to elaborate this concept a little further, referring to common clinical experience. It is a common observation that, following the anatomical changes that have occurred on the edentulous arches, the latter can demonstrate different degrees of resorption, which poses significant problems regarding the stability of the tissues adjacent to the ridge and/or the scanner's access to the regions to acquire. In these conditions (i.e. tissue instability, reduced accessibility), it is not surprising that intraoral scanning of edentulous arches is hardly practicable. In other words, the problem lies neither in a limitation of the scanning technology, nor in the absence of "features": simply, very often we find ourselves faced with areas that are difficult to access, where the topographic relationships of the ridges with structures and tissues mobile or unstable contiguous parts can heavily and negatively influence the intraoral scanning process. The solution to the problem, therefore, is based on the possibility of having access to the residual tissues of the edentulous ridge and keeping them stable for a period of time sufficient to complete the scan..
In tali condizioni (i.e. campo di scansione completamente libero e facilmente accessibile allo scanner, e tessuti contigui alla cresta stabilizzati), è possibile sfruttare interamente il potenzialle dello scanner e portare a termine la scansione intraorale di un'arcata edentula in pochi secondi. Per tale finalità sono stati sviluppati e brevettati degli strumenti ausiliari per la scansione intraorale delle arcate edentule (www.lorussoretractors.com), la cui azione è mostrata nelle figure 2 e 3.
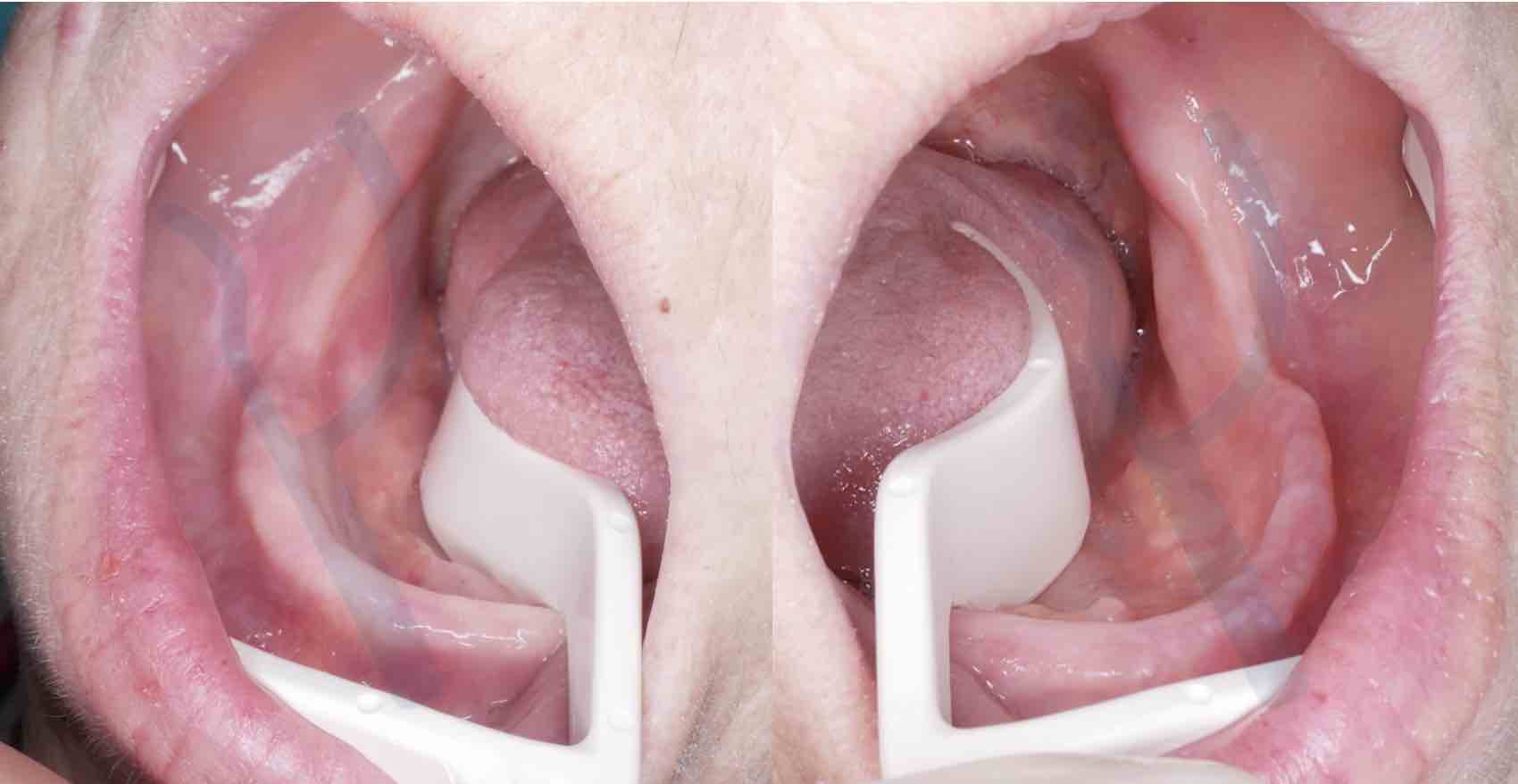
Figure 2: Tissue access and stabilization enabled by the Lo Russo Retractors® retractor system (www.lorussoretractors.com): mandibular arch fully accessible to the scanner up to the retromylohyoid fossa.

Figure 3: Lo Russo Retractors® in position on the upper arch: note the access and stabilization of the tissues in the vestibular area.
It is a system of retractors (Lo Russo Retractors®) which makes it possible to easily and effectively retract the tongue, lips and cheeks, thus freeing the scanning field (i.e. the edentulous ridge) and facilitating access to it from part of the scanner; furthermore, this system of retractors allows for efficient stabilization of the tissues adjacent to the ridge, simplifying the scanning process which becomes easy even for a single operator, and can be completed in a few seconds with consequent advantages also for the patient's comfort.
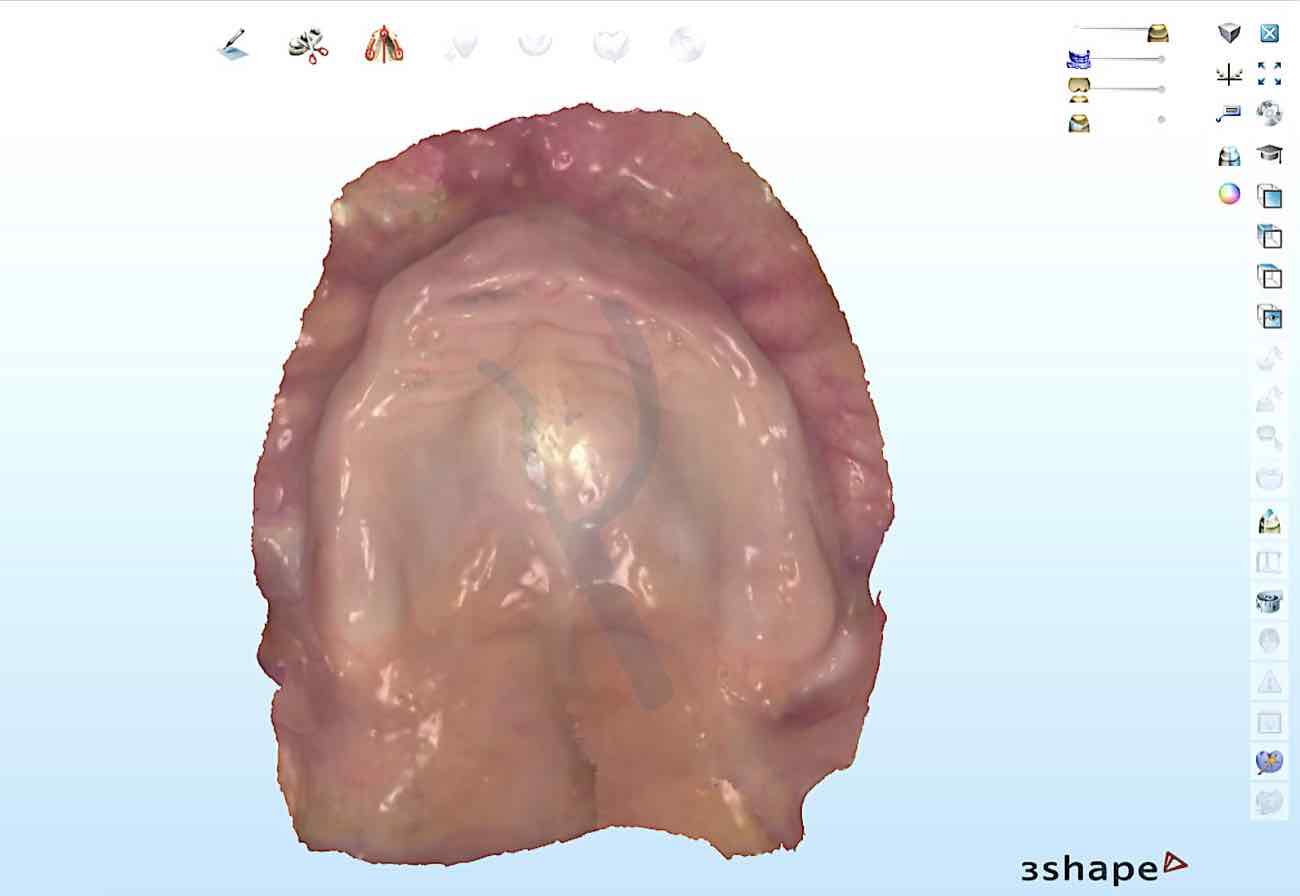
Figure 4: Intraoral scan of the arch in figure 3 ready for the design of the total prosthesis. Note the extension into the tuberosity and pterygomandibular raphe regions.
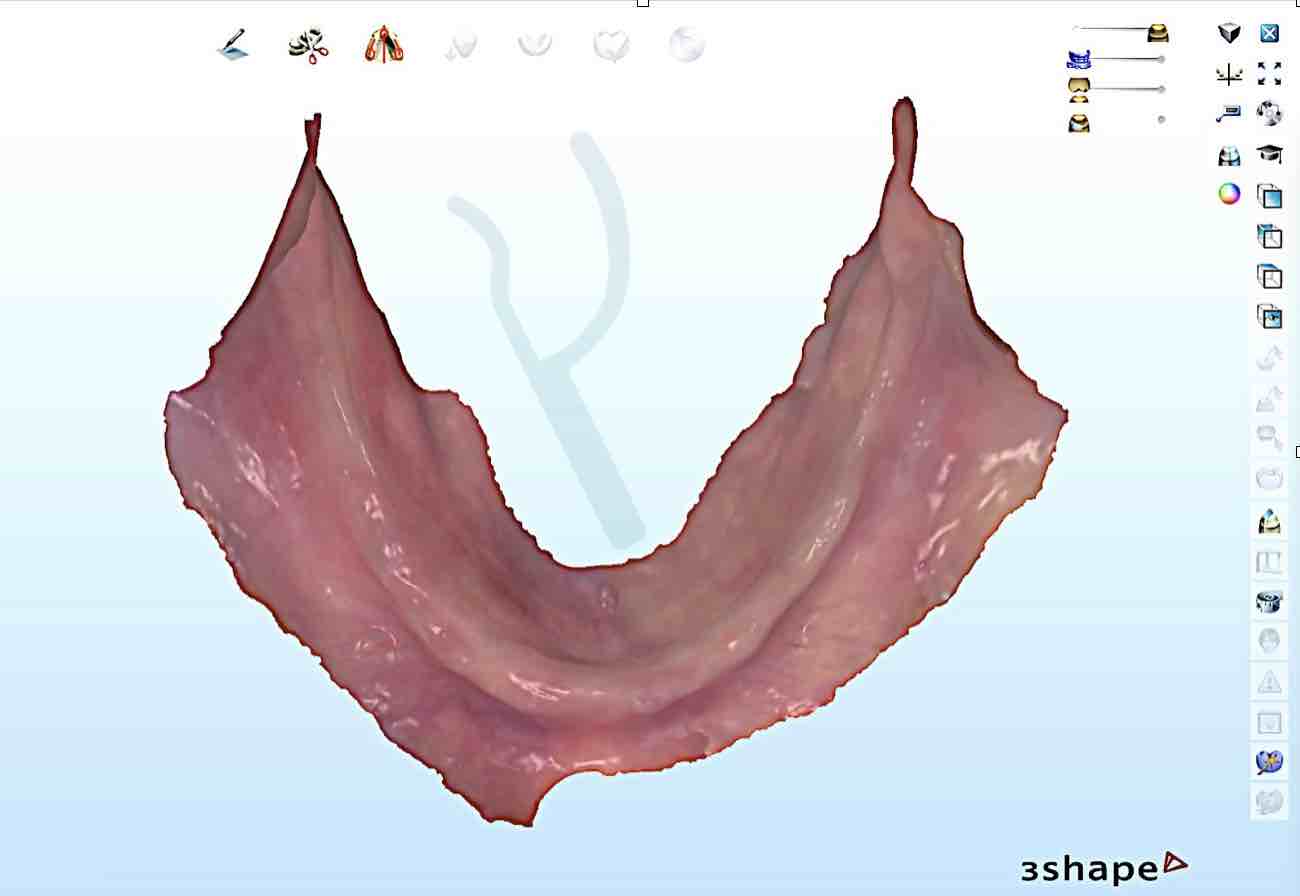
Figure 5: Intraoral scan of the mandibular arch carried out in the conditions of tissue retraction and stabilization represented in figure 2.
It seems clear that an adequate, fast and high-performance intraoral scanner remains an indispensable element, so the selection of scanning technology must be made by referring to those for which the effectiveness in the acquisition of edentulous arches has been demonstrated and validated. The 3Shape Trios 4 intraoral scanner was used in the images shown.
Likewise, an adequate understanding of the problem is a relevant prerequisite, the in-depth study of which remains desirable, together with the awareness and use of scanning strategies optimized for edentulous arches, the detailed description of which can be found in the following link: https://www.lorussoretractors.com/@/slides/strategie-di-scansione-delle-arcate-edentule-2
Having established that, with a high-performance scanner and adequate control of scanning conditions, intraoral scanning of edentulous arches is a feasible and predictable process, the accuracy of scans performed under these conditions and with the use of the aforementioned retractor system remains to be discussed. In vitro and in vivo studies have been published for some time now, reporting comparative data in terms of dimensional differences between intraoral scans of edentulous arches and corresponding impressions taken with a conventional technique. One of the few in vivo studies on the subject, with data relating to the edentulous mandibular arch (Lo Russo et al. J Prosthet Dent 2020;123:264-8), highlighted an average difference of approximately 30 microns for the maxillary arch and 20 for the mandibular arch. The same study clarified that this difference is not surprising, given the intrinsic characteristics of intraoral scanning and conventional impressions (i.e., 100% mucostatic vs. mucocompressive) and should absolutely not be attributed to an error or lack of accuracy in the intraoral scanning: it is simply a measure of mucosal resilience under the pressure applied by the impression material. The following images show a comparison between the intraoral scan obtained with the aforementioned retractor system (www.lorussoretractors.com) and the corresponding conventional impression.
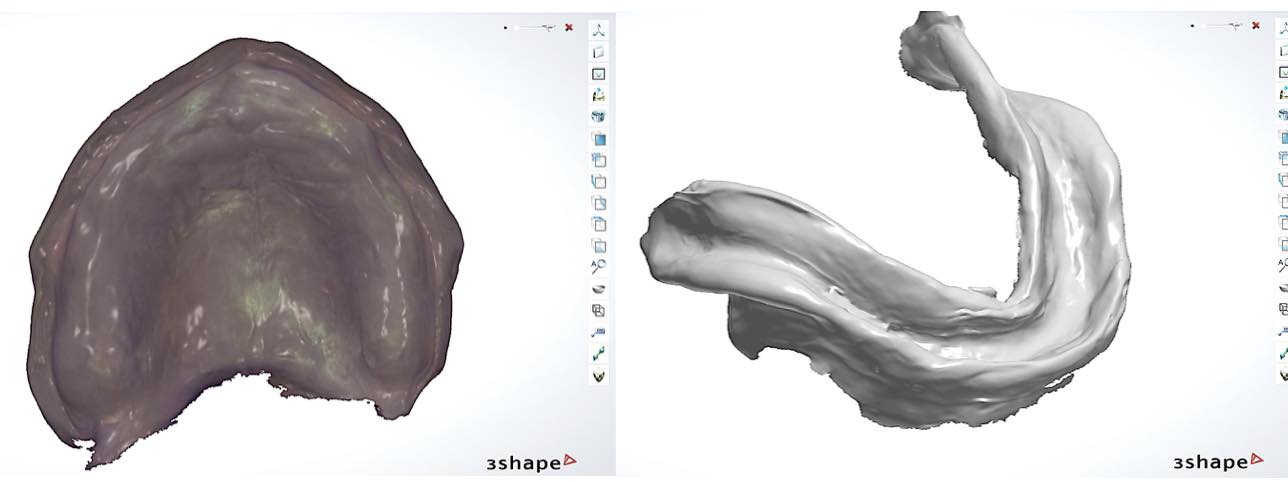
Figure 6: Conventional impressions corresponding to the intraoral scans shown in figures 4 and 5.
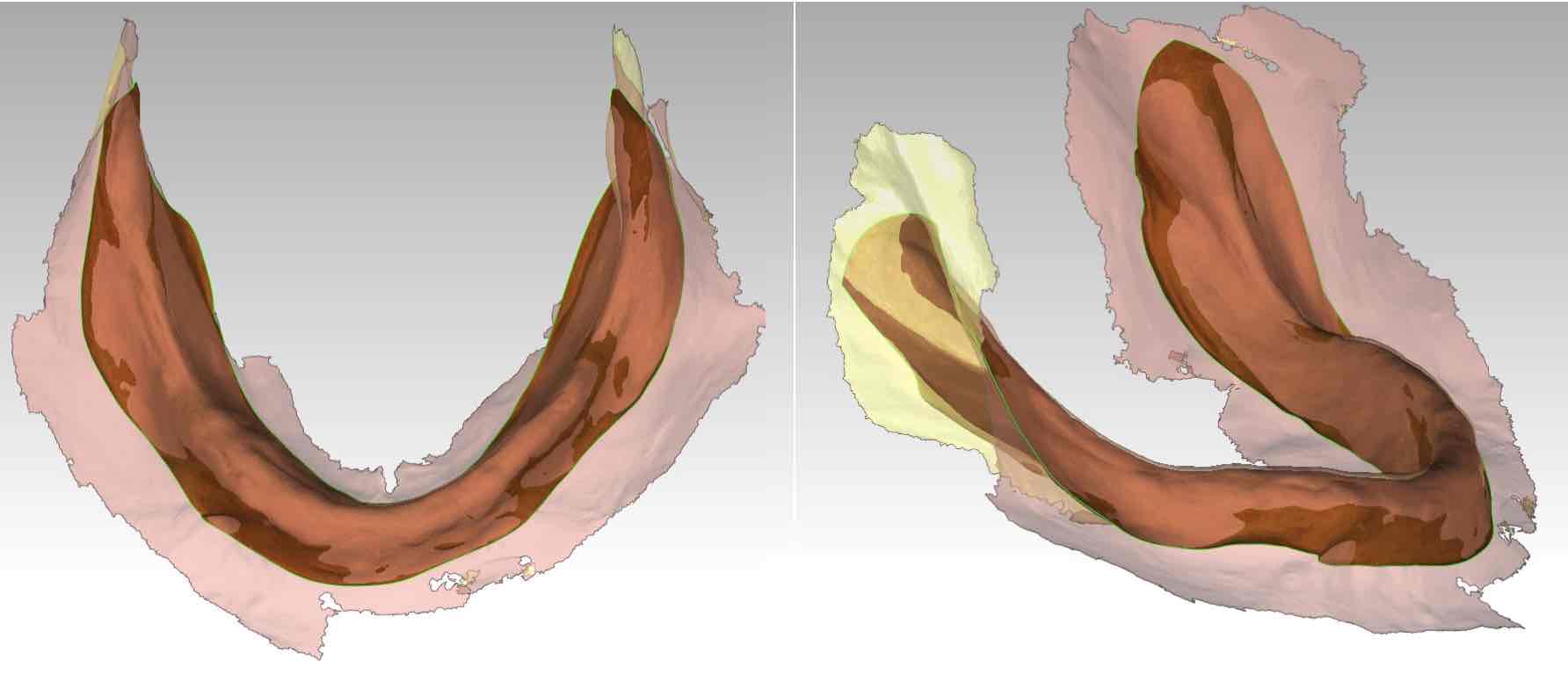
Figure 7: Intraoral scan and conventional impression superimposed and aligned.
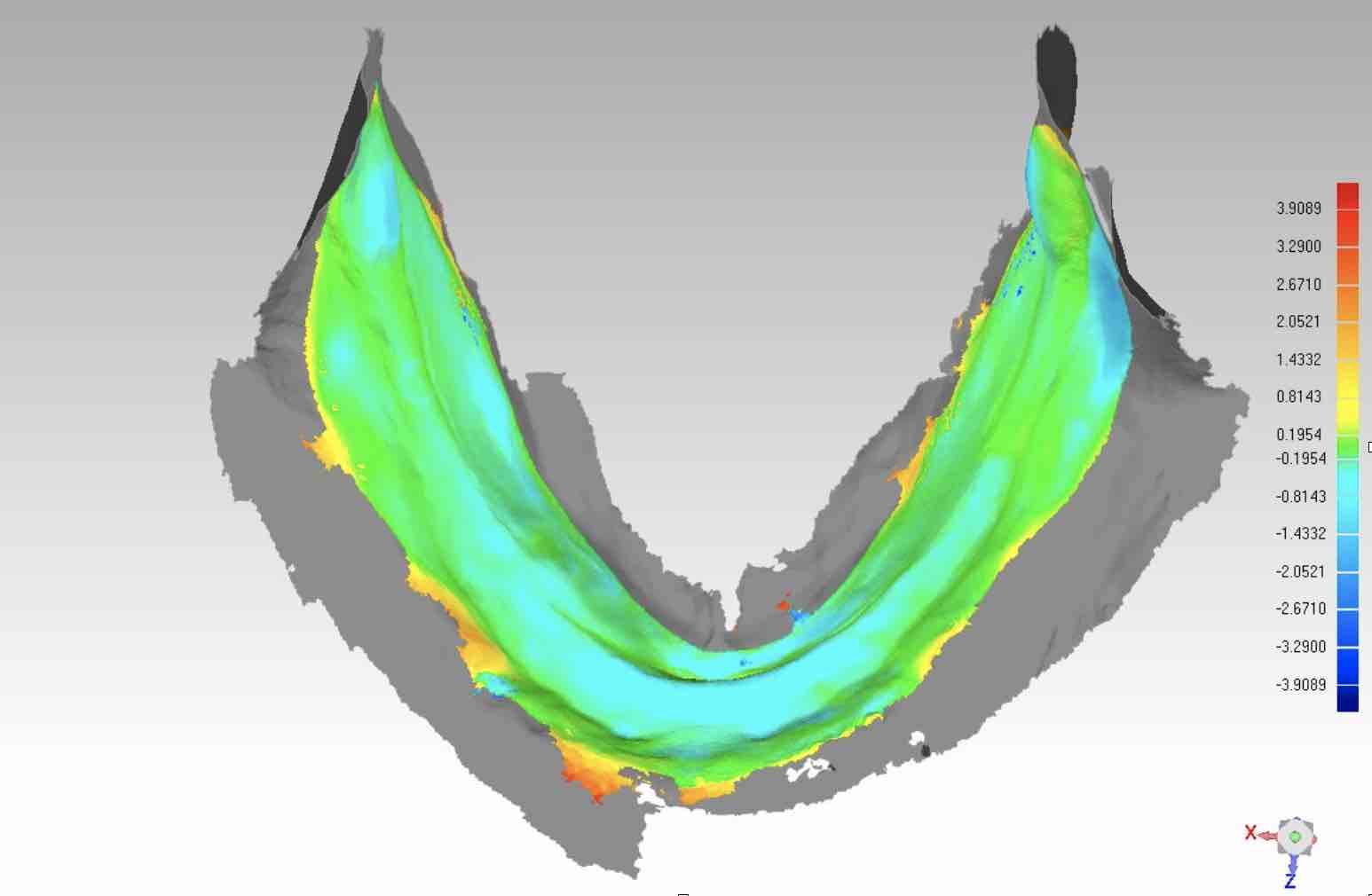
Figure 8: Color map of the differences between intraoral scan and conventional impression of the mandibular arch.
From the images it is possible to notice how: a) The extension of the intraoral scan is overextended (figure 7) compared to the mucocompressive impression obtained after edging. In particular, in figures 4 and 5 we can see how the acquisition of soft tissues extends well beyond and away from the edentulous ridges. b) Differences are measurable (figure 8), the meaning of which has already been discussed and clarified. c) No specific distortion patterns are observed.
In conclusion, the intraoral scanning technology currently available can express performances that allow the acquisition of soft tissues and edentulous ridges. This technology in association with the correct and effective control of clinical conditions (i.e. tissue retraction and their stabilization) allows efficient and accurate acquisition of the morphology of edentulous ridges for indications relating to removable or fixed implant-supported prostheses.