Introduction
Intraoral scanning of edentulous arches represents a procedure of great clinical relevance in prosthetic rehabilitation, both removable and fixed.
Direct digitization of fabrics allows you to operate in a completely digital environment, eliminating physical prints and models and improving:
- efficiency
- quality
- comfort for the patient
- standardization of clinical and laboratory procedures
However, doubts remain regarding:
- feasibility
- accuracy
- process predictability
What is the real problem in scanning edentulous people?
One of the main critical issues reported is the absence of “features” in the edentulous arches.
In reality, edentulous ridges present:
- macroscopic geometries (concavity and convexity)
- detectable surface textures
👉 This suggests that the problem is not simply a lack of geometry, but the preasons why scanning edentulous areas may fail are different.
Learn how to ensure accurate scanning of edentulous arches with dedicated tools
The role of surface geometry
As highlighted in the hard and soft palate scan, edentulous surfaces offer features that can be scanned.
👉 Under ideal conditions, therefore, scanning is technically possible.
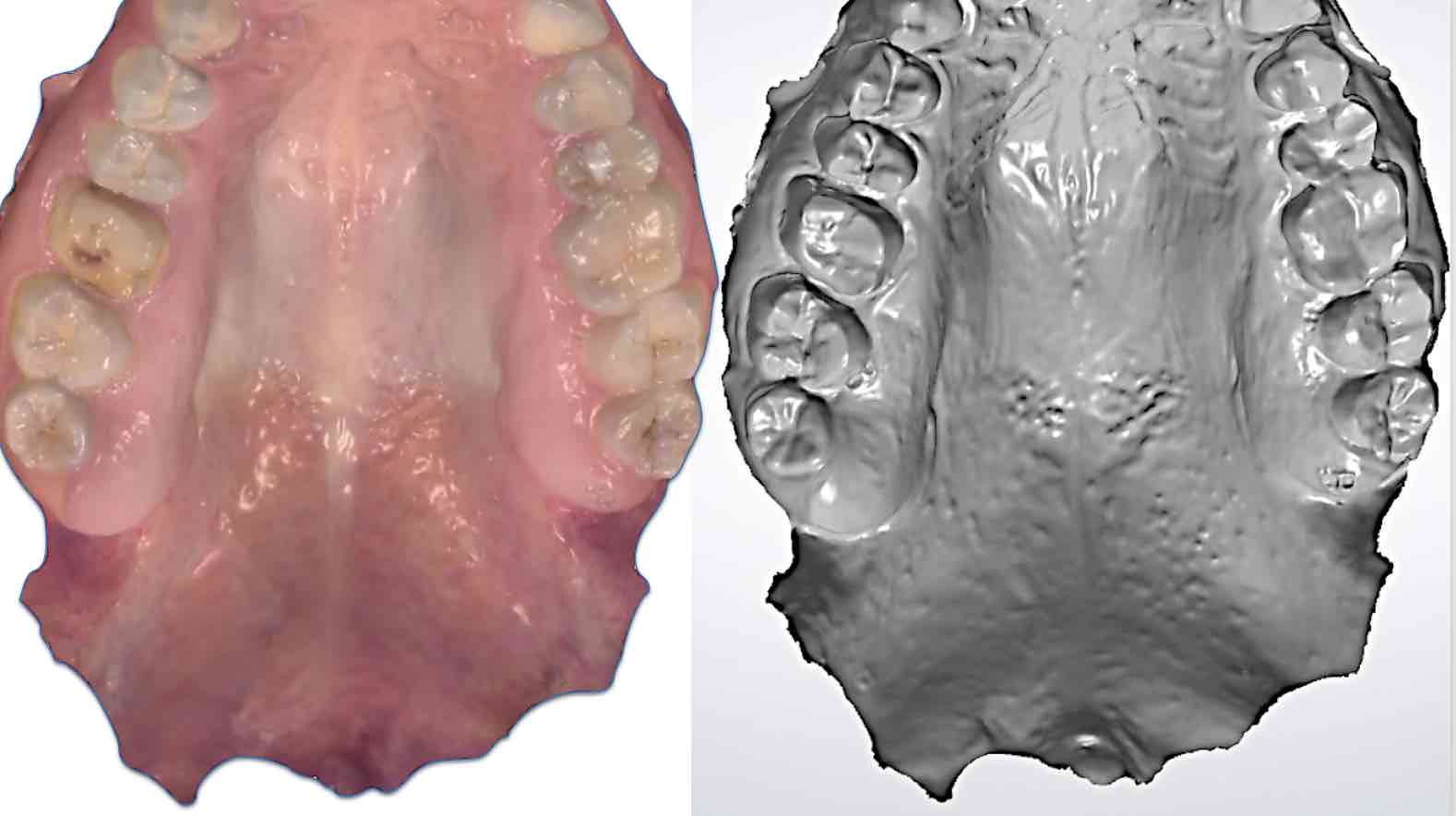
Figure 1: Scan of the soft palate; color manipulation makes macroscopic features and surface texture more evident.
Tissue access and stability: the real limit
Clinical experience shows that the real problem and common errors in intraoral scanning of edentulous arches are different:
👉 limited access and soft tissue instability
In the presence of:
- mobile tissues
- limited access
- complex anatomical conditions
the scan capturing becomes:
- difficult
- unstable
- not repeatable
👉 In short: the limitation is not the technology, but the clinical conditions. Poor access and tissue instability are the main causes of errors in intraoral scanning of edentulous patients, which can compromise the accuracy of the final result.
Landmarks: Solution or Complication?
The use of artificial landmarks (composites, cements, dedicated structures, or even landmarks requiring surgical procedures) has been suggested.
However:
- their effectiveness has not been definitively demonstrated
- they can complicate the procedure
👉 They do not necessarily represent the optimal solution.
How to improve intraoral scanning of edentulous patients
To obtain reliable results it is necessary:
- ensure complete access to the scanning field
- stabilize the tissues adjacent to the crest
- create controlled operating conditions
👉 Controlling clinical condition and workflow , as well as providing stabilization of movable tissues are key factors.
The role of tissue retraction and stabilization
In the presence of:
- free and sccessible scanning field
- stabilized tissues
it is possible:
- make full use of the scanner
- complete the scan in seconds
For this reason, dedicated tools have been developed such as the Lo Russo Retractors® retractor system, which allow:
- effective retraction of the tongue, lips and cheeks
- complete access to the edentulous ridge (figures 2 and 3)
- tissue stabilization
👉 This makes scanning easier, faster and more repeatable.
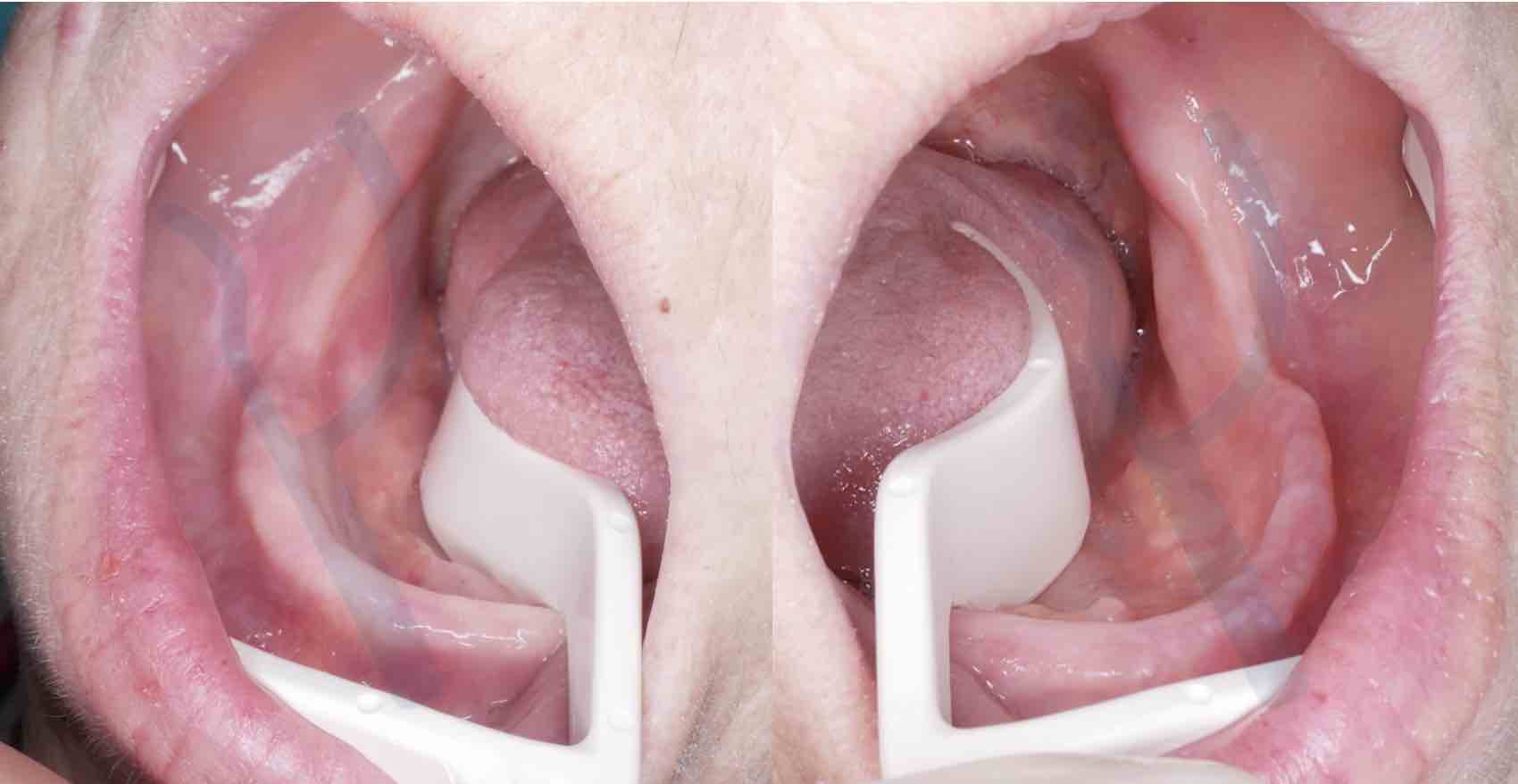
Figure 2: Tissue access and stabilization enabled by the Lo Russo Retractors® retractor system (www.lorussoretractors.com): mandibular arch fully accessible to the scanner up to the retromylohyoid fossa.

Figure 3: Lo Russo Retractors® in position on the upper arch: note the access and stabilization of the tissues in the vestibular area.
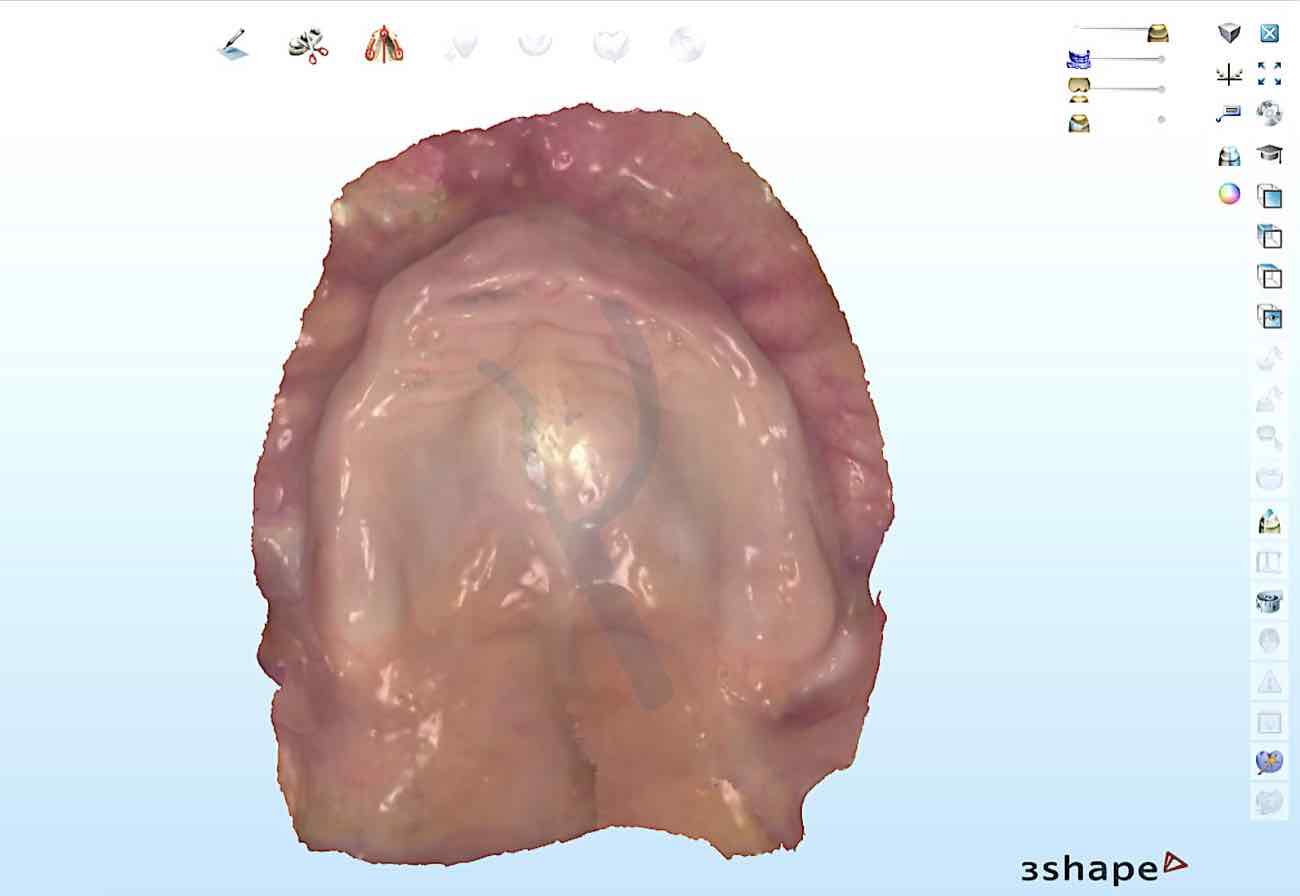
Figure 4: Intraoral scan of the arch in figure 3 ready for the design of the total prosthesis. Note the extension into the tuberosity and pterygomandibular raphe regions.
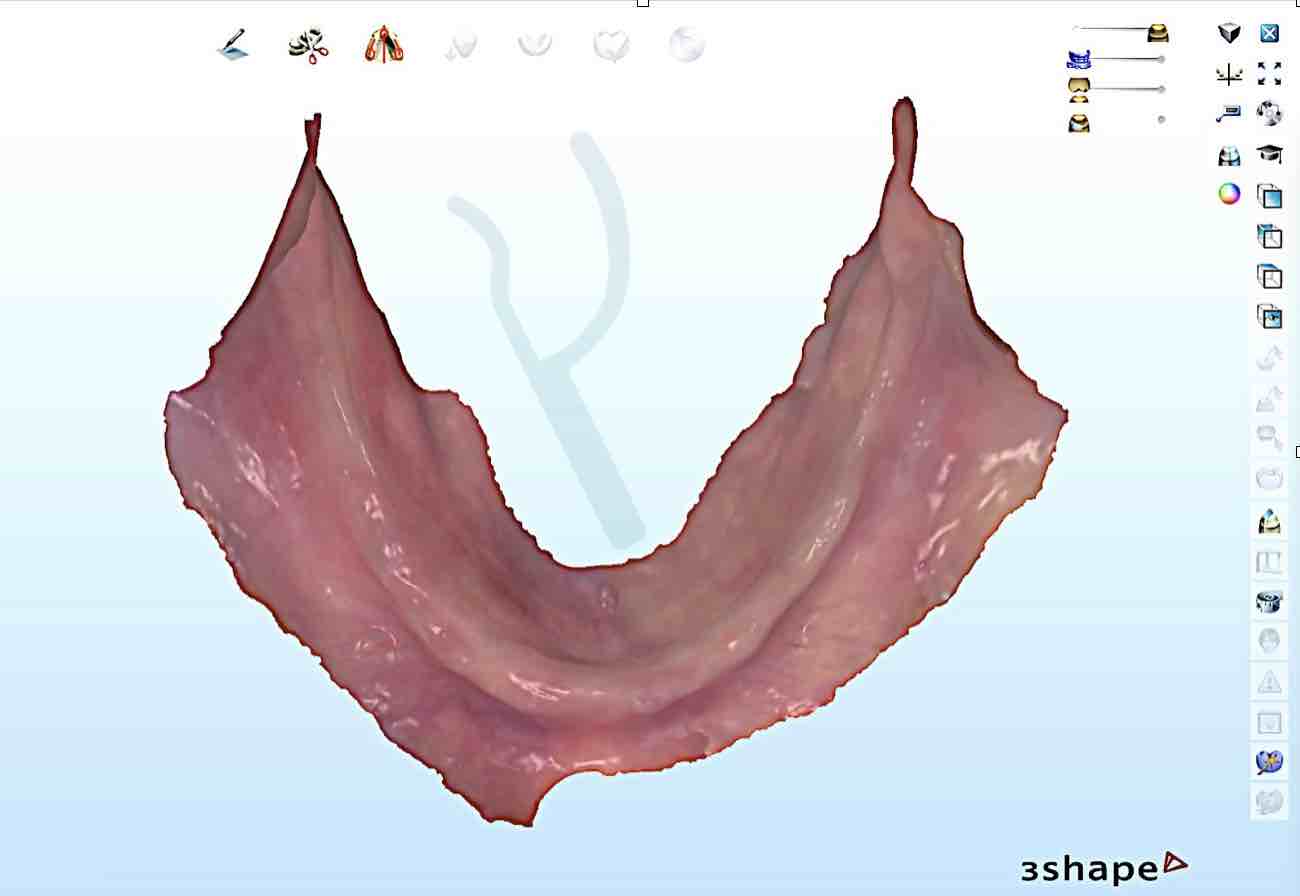
Figure 5: Intraoral scan of the mandibular arch carried out in the conditions of tissue retraction and stabilization represented in figure 2.
Accuracy of intraoral scanning in edentulous patients
In vitro and in vivo studies have compared:
- intraoral scanning of edentulous arches
- conventional impression
A clinical study (Lo Russo et al., J Prosthet Dent 2020) highlighted:
- ~30 microns for the maxillary arch
- ~20 microns for the mandibular arch
👉 These differences do not represent errors, but reflect:
- mucostatic behavior (digital intraoral scan)
- mucocompressive behavior (traditional impression based on impression materials)
In practice, this difference is simply a measure of mucosal resilience under the pressure applied by the impression material. The following images show a comparison between the intraoral scan obtained with the aforementioned retractor system (www.lorussoretractors.com) and the corresponding conventional impression.
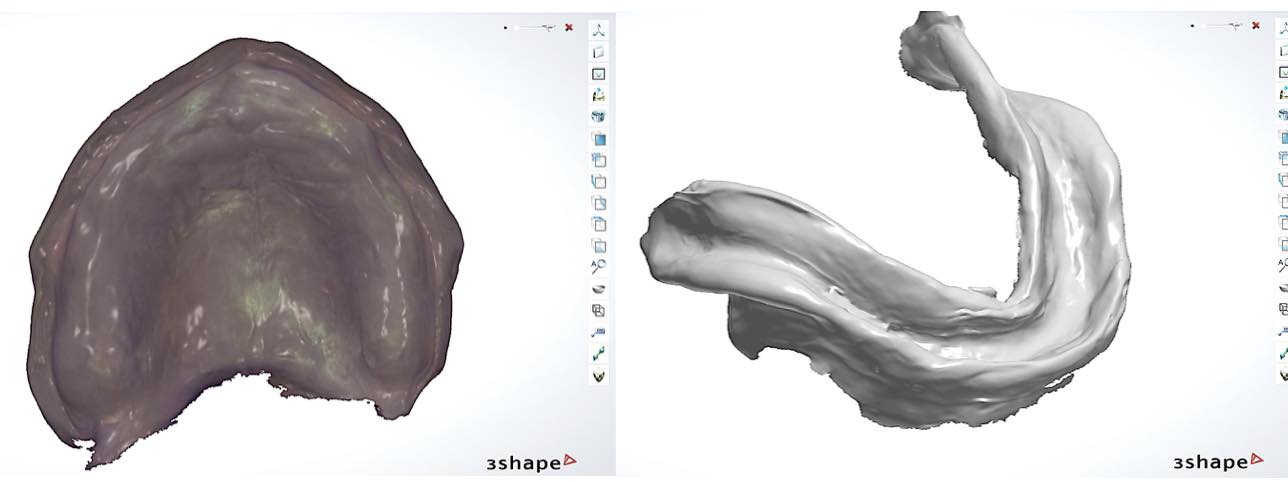
Figure 6: Conventional impressions corresponding to the intraoral scans shown in figures 4 and 5.
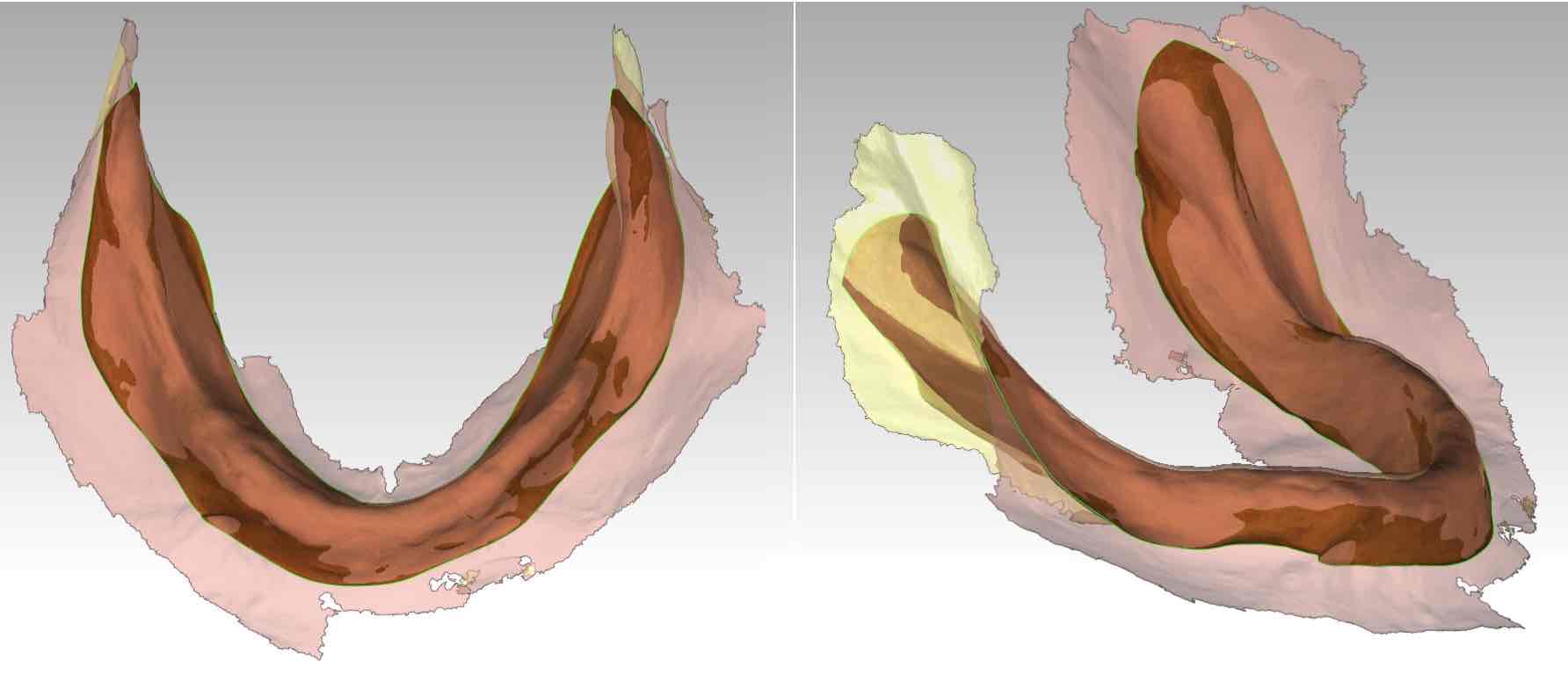
Figure 7: Intraoral scan and conventional impression superimposed and aligned.
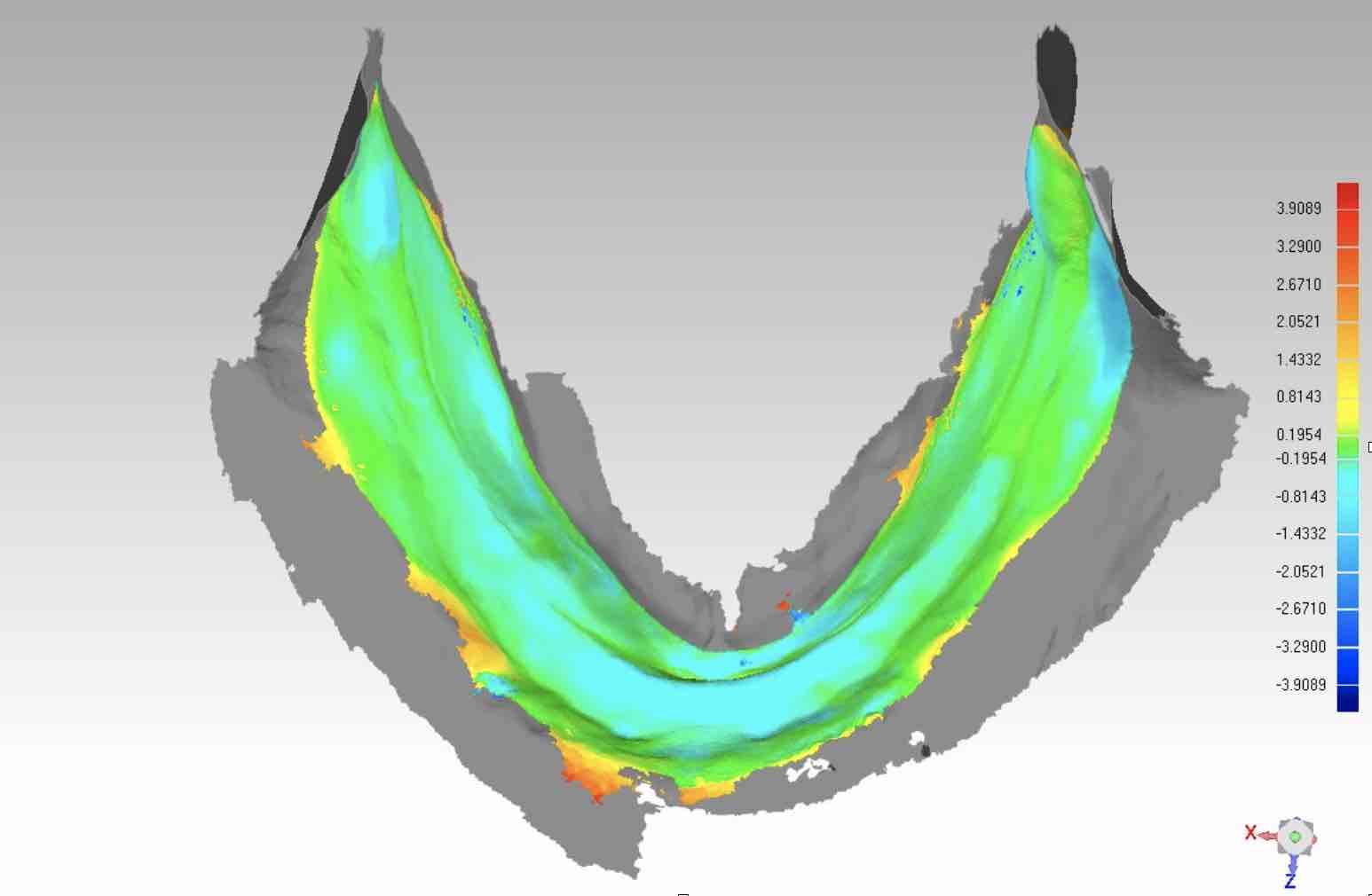
Figure 8: Color map of the differences between intraoral scan and conventional impression of the mandibular arch.
Analysis of the differences
The comparison shows that:
- intraoral scanning may be more extensive (figure 7)
- no significant distortion patterns are observed (figure 8)
- the differences are linked to the resilience of the tissues
👉 Digital technology is therefore reliable when used under correct conditions.
Conclusions
Digital technology is therefore reliable when used under correct conditions.
- feasible
- predictable
- clinically valid
👉 Provided that:
- high-performance scanners are used
- clinical conditions (correct management and stabilization of mobile tissues) are accurately controlled
- access and stability of the tissues are guaranteed
- validated scanning strategies are used
Under these conditions, digital represents an effective solution for the prosthetic rehabilitation of edentulous people, both with removable or fixed implant-supported treatment options.
Further information
For detailed operational strategies and insights into intraoral scanning for the rehabilitation of completely edentulous patients, see:
SCANNING STRATEGIES for edentulous arches